- LOGIN
- MemberShip
- 2026-07-05 23:34:30
- RSA's collateral period was reduced by 3 months
- by Lee, Hye-Kyung | translator Choi HeeYoung | 2020-11-26 08:38:52
The amount of collateral that pharmaceutical companies have to pay when signing an RSA drug is expected to decrease by 25%.
According to the 'Detailed Operation Guidelines for Drug Price Negotiation of the Risk Sharing Agreement' revised by The NHIS on October 8, the period of collateral has been changed from 12 months to 9 months.
This is because if the actual formula is substituted, the amount of collateral will decrease.

"Pharmaceutical companies have made a lot of requests to reduce the amount of collateral that is collectively entered at first," said Oh Se-rim, a team leader in the NHIS Drug Price Negotiation Department, who was in charge of announcing the revised matters.
Following that, Team leader Oh said, "It has been shown that the amount of collateral is arithmetically reduced by 25% by reducing the amount of collateral by three months from 12 months to 9 months." In the case of the Refund type, as the amount of collateral is reduced, it becomes 'estimated billing amount (maximum) x refund rate x 130%' to 'estimated billing amount (actual) x refund rate/1-refund rate x 9/12 x 130%'.
The reason that the estimated billing amount has changed from the upper limit (indicated price) to the actual price is that, while revising the guidelines, the 'actual fiscal impact criterion' was set in consideration of the refund of the estimated billing amount.
Based on the revised guidelines, if the amount of the collateral is calculated assuming a drug with a labeling price of ₩10,000, an actual price of ₩80,000, a refund rate of 20%, and an estimated billing volume of 1 million vials, it was previously '10 billion won (maximum amount) × 20% (refund rate) × It had to pay ₩2.6 billion as '130%', but '₩8 billion (actual) x 20%/(1-20%) (1-refund rate) x 9/12 x 130%' is applied as a change between collateral.
If so, it will reduce ₩650 million to ₩1.95 billion.
Team leader Oh explained, "The initial guideline was released and there was no change in the formula that was not in the refund rate part, but it was corrected by changing it to the actual price minus the refund rate.
There was a reduction in the amount of about 25%." Since its introduction in 2014, RSA has signed a total of 48 drugs and 85 items as of October 30.
By type, there are 13 Refund types (26 items), 18 Expenditure Cap types (29 items), 1 Refund type for initial treatment (2 items), and 3 Utilization Cap/Fixed Cost per Patient type (6 items), other type (1 item), and a combination of 12 items (21 items).
Expenditure Cap Change = According to the guidelines changed by The NHIS, the Expenditure Cap was changed from 130% to 100% of the estimated billing amount when negotiating the Article 6 risk sharing proposal.
At the time this guideline was published, the pharmaceutical industry was most opposed to it.
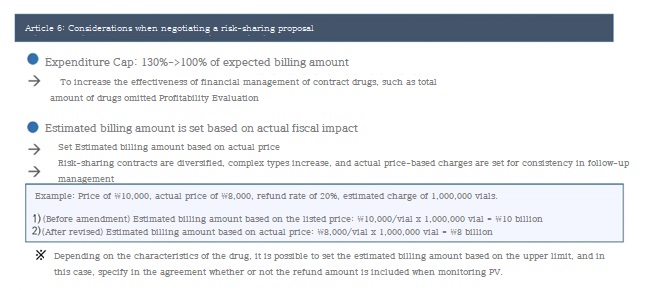
As a result of analyzing Expenditure Cap-type drugs, most of them have reached the 100% standard.
It will not have a big impact as expected." In addition, the standard of the estimated billing amount was changed from the upper limit to the actual price.
Depending on the nature of the drug, it is possible to set the estimated billing amount based on the upper limit amount, and when monitoring the Price-Volume (PV), they can specify whether the refund amount is included in the agreement.
Nam-seon Choi, Director of Drug Price Negotiations, said, "If we assume that an estimated billing amount of ₩20 billion and a refund of ₩5 billion, whether for initial treatment Refund or Utilization Cap/Fixed Cost per Patient, we will set ₩15 billion as the estimated billing amount." "Pharmaceutical companies can decide whether to set it based on the actual fiscal impact excluding the amount of refund or the details of the claim.“

"In the past, only one type was applied," said Choi, "a part that changed as the guidelines were revised and various types were mixed and the standard for the total amount was set together." He explained, "The principle is based on the actual price, but if the actual price cannot be made according to various types, it can be discussed in the negotiation and entered in the agreement." Expenditure Cap contract obligation for phase III conditionally licensed drugs = As risk-sharing targets expanded in this guideline, conditional drugs in phase III clinical trial were also included.
This drug will sign an Expenditure Cap contract, and team leader Oh interpreted, "For these drugs, it is not easy to submit profitability evaluation data, but the possibility of benefit registration may have increased" However, the definition of conditional drugs in phase III was specified in accordance with the 'Examination Regulations for Declaration of Product Permission for Drugs', and limited to drugs that were approved by submission of data for phase II and approved under the conditions of clinical data for phase III.
Team leader Oh said, "The drugs that have only partially submitted data on conditional drugs in clinical III or whose overall survival rate (OS) is released after approval are not considered conditional, but only drugs according to the review regulations." Expiration of contract term = One of the biggest changes from the revision of this guideline in The NHIS is the treatment method after the RSA contract term expires.
In the past, before the expiration of the RSA contract period (4+1 years), the NHIS requested the evaluation of the risk-sharing system of existing RSA drugs in the Pharmaceutical Benefits Advisory Committee of the HIRA However, only the changed guidelines do not allow the Pharmaceutical Benefits Advisory Committee to determine whether or not to be eligible for a risk-sharing system.
The clinical usefulness and cost-effectiveness of drugs near the expiration of the RSA contract will be evaluated.
And the NHIS will be able to re-contract or terminate the contract by negotiating risk-sharing plans such as the upper limit amount of the drug, the estimated billing amount and the refund rate, and the cap based on the result.
The NHIS, the parties to the contract, will have the overall risk-sharing contract.
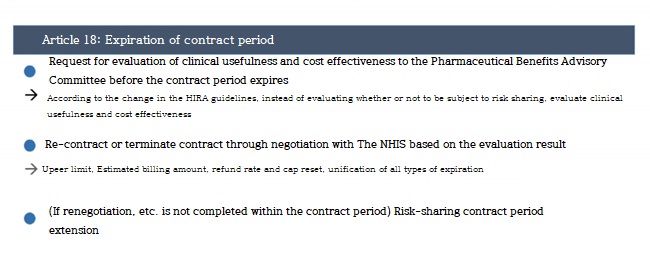
Team Leader Oh said, “The Leader decides whether to re-contract or negotiate based on the evaluation results of the HIRA, and continues the contract considering the upper limit amount, estimated billing amount, and refund rate in consideration of changes in the clinical environment over the past 4 to 5 years.
We will discuss whether or not with a pharmaceutical company."
-

- 0
댓글 운영방식은
댓글은 실명게재와 익명게재 방식이 있으며, 실명은 이름과 아이디가 노출됩니다. 익명은 필명으로 등록 가능하며, 대댓글은 익명으로 등록 가능합니다.
댓글 노출방식은
댓글 명예자문위원(팜-코니언-필기모양 아이콘)으로 위촉된 데일리팜 회원의 댓글은 ‘게시판형 보기’와 ’펼쳐보기형’ 리스트에서 항상 최상단에 노출됩니다. 새로운 댓글을 올리는 일반회원은 ‘게시판형’과 ‘펼쳐보기형’ 모두 팜코니언 회원이 쓴 댓글의 하단에 실시간 노출됩니다.
댓글의 삭제 기준은
다음의 경우 사전 통보없이 삭제하고 아이디 이용정지 또는 영구 가입제한이 될 수도 있습니다.
-
저작권·인격권 등 타인의 권리를 침해하는 경우
상용 프로그램의 등록과 게재, 배포를 안내하는 게시물
타인 또는 제3자의 저작권 및 기타 권리를 침해한 내용을 담은 게시물
-
근거 없는 비방·명예를 훼손하는 게시물
특정 이용자 및 개인에 대한 인신 공격적인 내용의 글 및 직접적인 욕설이 사용된 경우
특정 지역 및 종교간의 감정대립을 조장하는 내용
사실 확인이 안된 소문을 유포 시키는 경우
욕설과 비어, 속어를 담은 내용
정당법 및 공직선거법, 관계 법령에 저촉되는 경우(선관위 요청 시 즉시 삭제)
특정 지역이나 단체를 비하하는 경우
특정인의 명예를 훼손하여 해당인이 삭제를 요청하는 경우
특정인의 개인정보(주민등록번호, 전화, 상세주소 등)를 무단으로 게시하는 경우
타인의 ID 혹은 닉네임을 도용하는 경우
-
게시판 특성상 제한되는 내용
서비스 주제와 맞지 않는 내용의 글을 게재한 경우
동일 내용의 연속 게재 및 여러 기사에 중복 게재한 경우
부분적으로 변경하여 반복 게재하는 경우도 포함
제목과 관련 없는 내용의 게시물, 제목과 본문이 무관한 경우
돈벌기 및 직·간접 상업적 목적의 내용이 포함된 게시물
게시물 읽기 유도 등을 위해 내용과 무관한 제목을 사용한 경우
-
수사기관 등의 공식적인 요청이 있는 경우
-
기타사항
각 서비스의 필요성에 따라 미리 공지한 경우
기타 법률에 저촉되는 정보 게재를 목적으로 할 경우
기타 원만한 운영을 위해 운영자가 필요하다고 판단되는 내용
-
사실 관계 확인 후 삭제
저작권자로부터 허락받지 않은 내용을 무단 게재, 복제, 배포하는 경우
타인의 초상권을 침해하거나 개인정보를 유출하는 경우
당사에 제공한 이용자의 정보가 허위인 경우 (타인의 ID, 비밀번호 도용 등)
※이상의 내용중 일부 사항에 적용될 경우 이용약관 및 관련 법률에 의해 제재를 받으실 수도 있으며, 민·형사상 처벌을 받을 수도 있습니다.
※위에 명시되지 않은 내용이더라도 불법적인 내용으로 판단되거나 데일리팜 서비스에 바람직하지 않다고 판단되는 경우는 선 조치 이후 본 관리 기준을 수정 공시하겠습니다.
※기타 문의 사항은 데일리팜 운영자에게 연락주십시오. 메일 주소는 dailypharm@dailypharm.com입니다.
- [Reporter's View] CSO Association set to receive official legal status
- Reporter's view | Kim, Jin-Gu

- "CHE, limitations of steroids…attention is now focused on 'Anzupgo'"
- Reporter's view | Son, Hyung Min