- LOGIN
- MemberShip
- 2026-06-13 20:42:36

- Policy
- CSO 규제 향방은…복지부, 재위탁·수수료율 손질 가능성
- by Lee, Jeong-Hwan May 26, 2026 03:21pm
- [데일리팜=이정환 기자] 보건복지부가 의약품 판촉영업 대행사(CSO) 추가 규제를 통한 의약품 유통 구조 투명성 강화 필요성을에 공감하면서 이어질 정책 방향에 시선이 모인다.제약업계에서 회자되고 있는 규제는 CSO가 다른 CSO에게 의약품 영업판촉 업무를 재위탁하는 행위를 금지하거나 관련 규제 수위를 지금보다 높이는 방식이다.이와 함께 CSO가 제약사에게 요구하는 수수료율의 상한선을 규정하는 등 CSO 수수료에 대한 행정적·법적 제한을 신설하는 규제도 거론되고 있다.25일 제약업계는 복지부가 한국제약바이오협회와 함께 CSO 실태조사에 착수한 만큼 연내 구체적인 규제 방향성을 수립할 것으로 전망중이다.현재 CSO 업계는 제약바이오산업 육성을 위해 CSO도 산업으로 육성할 필요성을 강조하며 복지부를 향해 한국CSO협회의 사단법인 인가를 촉구하는 실정이다.반면 복지부와 국내외 제약사들은 CSO의 사단법인 인가는 아직 시기상조라는 입장이다. CSO 업계가 CSO협회를 조직해 자체적으로 산업 선진화 등 노력을 기울이고 있지만, 여전히 CSO를 활용한 불법이 정화되지 않는 등 사단법인으로서 지위를 인정해주기엔 역부족이라는 평가다.이에 복지부와 제약협회 실태조사 이후 추가 규제가 이뤄져야 논의 가능성이 향상할 것으로 보인다.일단 CSO를 악용한 불법 리베이트의 가장 실질적인 원인으로 꼽히는 '무제한 재위탁'이 규제 사정권으로 분류된다.제약사가 CSO에게 의약품 판촉영업 대행 위수탁 계약을 체결한 이후, 해당 CSO가 다른 CSO와 또 위수탁 계약을 체결하면서 불법 리베이트 진원지를 찾을 수 없는 문제를 해결할 필요가 있다는 게 복지부와 제약업계, 국회의 공감대다. CSO 위탁 계약 원천 금지 규제 가능성이 거론되는 이유다.다음으로는 제약사가 CSO에 지급하는 의약품 판촉영업 수수료 비중을 제한하는 수수료 상한제다. 높은 CSO 수수료는 결국 불법 의약품 리베이트 재원으로 쓰이게 된다는 비판을 법으로 규제하는 차원이다.다만 CSO 수수료 규제는 헌법에 위배될 소지가 있어 복지부와 정치권은 입법에 고심하는 표정이다. 그럼에도 CSO 수수료 제한이 실질적인 리베이트 근절과 투명한 의약품 유통질서 강화 효과가 기대될 경우 간접적으로 CSO 수수료 구조를 투명화하는 행정 규제와 입법이 추진될 공산이 크다.복지부는 일단 이번 실태조사에서 제약사와 CSO, CSO와 CSO 간 위수탁 계약, 재위탁 계약 현황 분석으로 규제 방향성을 수립한다는 방침이다.특히 복지부는 CSO 산업을 육성하는 게 복지부의 주된 업무가 아니라는 입장으로, 공정하고 투명한 의약품 유통질서 확립 즉, CSO 리베이트 근절을 위한 규제 신설을 고민할 것으로 보인다.제약업계 관계자는 "복지부는 CSO 수수료율 규제를 정부가 나서서 추진하는 것에 일부 부담감을 느끼는 동시에 위헌 가능성에 집중하는 분위기"라며 "법으로 CSO 수수료율을 옭아매는 게 무조건 좋은 방법인지 여부에 대한 판단도 안 선 것 같다. 다만 재위탁 문제가 심각해 불법 리베이트 규제 공백을 키우고 있는데 대한 문제의식엔 공감하는 것으로 안다"고 귀띔했다.그러면서 "CSO 수수료 상한제는 제약사들로서는 가장 직접적이고 효율적인 규제 방향일 수 있다. 하지만 법으로 당장 제한하기 어려울 수 있어 간접적으로 CSO가 과도한 수수료를 제약사에 요구하고 정당한 판촉이 아닌 리베이트 영업으로 품목 처방 매출을 유지하는 문제를 막는 방법을 고민할 필요가 있다"며 "CSO 업계 자체도 일단 자정 필요성에 공감은 하고 있는 것으로 안다. 문제는 너무 점 조직으로 구성돼 CSO 업계에 대한 일괄적 규제나 의견 수렴, 통합이 어렵다는 게 문제"라고 말했다.이어 "일단 불법 리베이트 근절에 앞장서고 있는 다수 제약사는 CSO 신고제 시행 2년차를 맞은 지금, 신고제를 넘어선 추가 규제가 필요하다는 의견"이라며 "복지부의 제네릭 약가인하 정책이 예고된 시점과 맞물려 추가 행정이 시급하다"고 덧붙였다.
- Policy
- Korea approves Keytruda SC, developed with Alteogen's technology
- by Lee, Tak-Sun May 21, 2026 10:15am
- Product photo of KeytrudaThe subcutaneous (SC) formulation of 'Keytruda (pembrolizumab),' a global blockbuster immunotherapy for cancer treatment, is set to enter the Korean market after securing marketing authorization from the Ministry of Food and Drug Safety (MFDS). This approval is evaluated as a major achievement for the domestic biopharma industry, as the product integrates Alteogen's platform technology, and Samsung Biologics has been confirmed as part of the global contract manufacturing organization (CMO) lineup.On the 19th, the MFDS granted official marketing authorization for MSD Korea's 'Keytruda SC Inj (recombinant).'The newly approved Keytruda SC was developed using ALT-B4, a modified human hyaluronidase platform technology from the domestic biotech company Alteogen. It features a formulation combining the active ingredient, pembrolizumab, with 'berahyaluronidase alfa,' an enzyme that temporarily degrades the extracellular matrix of subcutaneous tissue. Using this technology, the existing intravenous (IV) formulation was converted into an SC formulation, enabling rapid dispersion and permeation of the drug into subcutaneous tissue.The contribution of South Korean companies is also significant in the manufacturing sector. According to the MFDS approval details, Keytruda SC's global contract manufacturing network includes Samsung Biologics, Korea's largest CMO, alongside BSP Pilot, Boehringer Ingelheim, and MSD headquarters. This system has enabled an innovative new drug developed with Korean platform technology to be supplied globally through Korea's state-of-the-art manufacturing facilities.Patient convenience is expected to improve dramatically. With the conventional Keytruda IV formulation, patients had to spend 30 minutes to an hour receiving an infusion in a hospital infusion center bed. In contrast, Keytruda SC can be administered by healthcare professionals into the thigh or abdomen in just one to two minutes. The dosing schedule can be selected based on the patient's condition, offering options for either a 3-week cycle (395 mg) or a 6-week cycle (790 mg). Patients currently receiving the IV formulation can also transition to the SC formulation starting with their next scheduled dose, which is expected to yield strong preference in clinical settings.The approved indications include the extensive scope of the existing IV formulation. Keytruda SC secured approvals across a total of 18 cancer types, including ▲melanoma ▲non-small cell lung cancer (NSCLC) ▲malignant pleural mesothelioma ▲head and neck cancer, classical Hodgkin lymphoma ▲urothelial carcinoma, gastric cancer ▲esophageal cancer ▲renal cell carcinoma, endometrial carcinoma ▲triple-negative breast cancer (TNBC) ▲cervical cancer ▲biliary tract cancer ▲hepatocellular carcinoma ▲microsatellite instability-high (MSI-H) solid tumors. This approval is based on data from a large-scale global bioequivalence clinical trial (MK-3475A-D77), which demonstrated comparable pharmacokinetic (PK) properties, efficacy, and safety profiles to the IV formulation.A pharmaceutical industry employee stated, "Keytruda is a mega-blockbuster competing for the top spot in global sales," and added, "The fact that Alteogen's technological advancement and Samsung Biologics' manufacturing capabilities have been integrated into global pharma giant MSD's core pipeline is a major milestone, demonstrating that the standing of the Korean pharma and biotech industry has taken a significant leap forward." Keytruda is a mega blockbuster that recorded global sales of KRW 46 trillion last year. In South Korea, Keytruda's sales have surpassed KRW 500 billion, ranking as the highest-performing pharmaceutical in the country.

- Policy
- Generic market for anti-cancer drug Xtandi heats up
- by Lee, Tak-Sun May 20, 2026 02:28pm
- Original Xtandi TabThe generic market for Xtandi (enzalutamide, Astellas), a blockbuster prostate cancer treatment, is in turmoil.With the expiration of the substance patent approaching this June and approvals for soft capsule generics coming one after another, latecomers are now setting their sights squarely on the ‘tablet’ market—the original manufacturer’s latest strategic weapon— rapidly expanding the competitive battlefield.According to industry sources, on April 24, applications for approval of three film-coated tablet strengths of enzalutamide (40mg, 80mg, and 160mg) were simultaneously submitted to the Ministry of Food and Drug Safety. Industry attention is focused on these applications because they aim to secure ‘first generic exclusivity,’ considered the key to early market dominance.From capsules to tablets…follow-up approvals accelerate after breaking the 2033 barrierOriginally, the Xtandi generic market had been developing primarily around soft capsule formulations timed with the expiration of the substance patent on June 27. Major pharmaceutical companies, including Alvogen Korea, Daewon Pharmaceutical, Hanmi Pharmaceutical, GL Pharma, and Dongkook Pharmaceutical, have already obtained approvals for soft capsule generics and are preparing to launch.In response, original manufacturer Astellas Pharma Korea introduced ‘Xtandi Tab’ (40mg and 80mg) with improved dosing convenience and completed reimbursement listing last April. This was part of a defensive strategy to shift the market’s center of gravity toward tablets and fend off the generic competition. This was because the tablet formulation was protected by a separate composition patent valid until September 2033.However, the defensive line collapsed as domestic pharmaceutical companies successively succeeded in circumventing this 2033 formulation patent through a series of negative scope confirmation trials. The latest film-coated tablet generic applications are therefore interpreted as the first step toward realizing a ‘dual competition’ structure between dosage forms after neutralizing the patent barrier.Addition of a 160mg high-dose option… Aiming for exclusivity through first generic approval rightsA notable feature of the film-coated tablet lineup applied for this time is the inclusion of a 160mg high-dose product, which is not available in the original Xtandi Tab lineup (40mg, 80mg).Currently, patients face the inconvenience of having to take four 40mg soft capsules at once each day. In response to the original manufacturer introducing an 80mg tablet form to reduce the number of pills taken to two, the generic manufacturer has launched a counterattack by developing a 160mg ultra-high-dose formulation that requires taking “just one pill a day.” This is a strategy to surpass the original in terms of convenience.Furthermore, if these companies secure first generic exclusivity based on the latest applications, they will gain the privilege of blocking other tablet generics from entering the market for a certain period while competing exclusively against the original product.A pharmaceutical industry official predicted, “If the ‘first war’ takes place in June when soft capsule generics flood the market immediately after the substance patent expires, then approvals and reimbursement listings for tablet generics pursuing first generic exclusivity will ignite the ‘second war’ in the second half of the year.”As a direct confrontation approaches between the original company’s market-defense strategy through tablet conversion and domestic pharmaceutical firms seeking early dominance of the tablet market through patent circumvention and independent high-dose lineups, the industry’s attention is focused on who will take the lead in the enzalutamide market. Xtandi recorded domestic sales of KRW 38 billion last year, according to UBIST data.

- Policy
- MFDS to maintain small-packaging drug regulations
- by Lee, Tak-Sun May 20, 2026 02:28pm
- The Ministry of Food and Drug Safety has recommended that pharmaceutical companies voluntarily adjust their own packaging practices rather than granting the industry’s request to relax small-packaging regulations due to stable drug supply concerns arising from the Middle East conflict. The move is interpreted as maintaining the small-packaging regulations while expanding recognition of exceptional cases. Industry requests for a grace period on administrative penalties this year appear to have been rejected following opposition from pharmacy organizations and related groups.This is interpreted as the government’s intention to expand the recognition of exceptions while maintaining compliance with the small-packaging regulations. It is analyzed that the industry’s initial request for a suspension of administrative penalties this year was rejected due to opposition from groups such as the Korean Pharmaceutical Association.According to industry sources on the 18th, the MFDS recently sent an official notice to pharmaceutical associations requesting that each pharmaceutical company voluntarily adjust small-package supply ratios.Under the current “Regulations on Supply of Pharmaceuticals in Small Packaging Units,” pharmaceutical manufacturers and importers are required to supply at least 10% of their annual production or import volume to pharmacies in small packaging units.The standards are set at 30 tablets or fewer for bottle packaging, 100 tablets or fewer for blister packs, and 500 mL or less for syrups. Violations result in administrative penalties such as suspension of sales operations.The mandatory small-packaging rule was originally introduced to reduce excessive inventory at pharmacies and the resulting social costs from the disposal of unused stock.Recently, the pharmaceutical industry requested relaxation of the small-packaging regulations due to shortages of pharmaceutical packaging materials caused by instability in naphtha supply stemming from the Middle East conflict. In particular, the industry requested suspension of administrative penalties this year, even if mandatory small-package production ratios were not met.On the 2nd of last month, MFDS Minister Yu-Kyoung Oh visited JW Pharmaceutical to inspect IV solution packaging and announced that the ministry would swiftly pursue proactive administrative measures, including the relaxation of the small-packaging obligations.Following this, the MFDS working-level department reviewed the potential easing of the small-packaging requirement. However, pharmacy organizations, including the Korean Pharmaceutical Association, opposed such measures, citing concerns such as inventory disposal, making policy decisions difficult.Ultimately, it appears the MFDS has decided to adhere to the regulations while actively utilizing exceptions.In an official notice, the MFDS stated, “The MFDS has recommended that pharmaceutical companies voluntarily reduce the use of drug packaging materials, such as by adjusting the ratio of small-volume packaging.”The ministry added, “While complying with the minimum standards for small-package supply in consideration of the purpose and intent of the ‘Regulations on Supply of Pharmaceuticals in Small Packaging Units,’ if compliance becomes difficult due to shortages in packaging material raw supplies caused by wartime conditions, companies may submit statements on product-specific explanations and supporting materials to the MFDS under Article 5 of the regulation to receive exemption from the small-package requirements.”The measure is ultimately interpreted as maintaining the small-package supply obligation while broadly recognizing exception products.A pharmaceutical industry official stated, “In response to opposition from the Korean Pharmaceutical Association and others, it appears that the request for a suspension of administrative penalties requested by the industry has not been accepted. However, the MFDS’s request for voluntary adjustment by pharmaceutical companies can be interpreted as an intention to actively recognize exceptions.”
- Policy
- SK plasma gains approval for Revolade generic
- by Lee, Tak-Sun May 20, 2026 02:28pm
- Original drug, Novartis’ ‘Revolade’SK Plasma has officially entered the generic market for Novartis’ rare disease treatment Revolade (eltrombopag olamine). Following Pharmbio Korea, which first entered the market, SK Plasma is joining as a latecomer, turning the competition among domestic generic manufacturers into a two-way race.On the 18th, the Ministry of Food and Drug Safety approved two dosage strengths (25mg and 50mg) of SK Plasma’s thrombocytopenia and severe aplastic anemia treatment, “Revolpag Tab.”The original drug for Revolpag is Novartis Korea’s ‘Revolade.’ The indications SK Plasma received approval for this time include all key efficacy and indication areas held by the original drug.The three approved indications include: ▲Treatment of thrombocytopenia in chronic immune (idiopathic) thrombocytopenia patients who showed insufficient response to corticosteroids or immunoglobulins; ▲ Treatment of thrombocytopenia to initiate and maintain interferon-based therapy in chronic hepatitis C patients, and as ▲First-line treatment of severe aplastic anemia in pediatric patients aged 2 years and older and adults in combination with immunosuppressive therapy, as well as treatment of severe aplastic anemia unresponsive to prior therapies.However, for chronic immune thrombocytopenia and chronic hepatitis C treatment, the drug is approved only for use in clinical conditions associated with increased bleeding risk and cannot be used for the purpose of normalizing platelet counts.Previously, SK Plasma successfully circumvented three “new pharmaceutical composition” patents that had served as the core barrier protecting Revolade, winning a negative scope confirmation trial after a dispute that went all the way to the Supreme Court. This approval was achieved after fully resolving patent risks.As a result, the domestic eltrombopag olamine market is expected to enter an intense competitive phase between Pharmbio Korea’s first-mover product “Elpag Tab” and SK Plasma’s late-entry “Revolpag Tab.” Elpag launched in October 2024.The Revolade market has continued to grow after reimbursement criteria were expanded in 2024, reaching import sales of approximately USD 5.23 million (around KRW 7.8 billion).A pharmaceutical industry official commented, “With Pharmbio Korea already in the market and expanding its market share, SK Plasma has secured approval and is leveraging its full indication coverage. Once reimbursement listing and pricing procedures are completed and the product launches in earnest, treatment options for physicians and patients will expand significantly.”

- Policy
- Darzalex SC and Omjjara complete drug price negotiations
- by Jung, Heung-Jun May 19, 2026 11:08am
- Janssen Korea’s multiple myeloma treatment, Darzalex SC (daratumumab), is expected to be listed for reimbursement after completing drug price negotiations with the National Health Insurance Service.In addition, Korea GSK’s new myelofibrosis treatment Omjjara Tab (momelotinib) 100mg, 150mg, and 200mg has also reached a pricing agreement and will enter reimbursement listing.According to industry sources on the 18th, Darzalex SC and Omjjara Tab, which entered negotiations with the NHIS in March, recently finalized pricing agreements.Both drugs are new therapies that passed the Drug Reimbursement Evaluation Committee in January. Darzalex SC was recognized as appropriate for reimbursement as “combination therapy with bortezomib, cyclophosphamide, and dexamethasone in newly diagnosed light-chain amyloidosis patients.”Unless unexpected issues arise, both drugs are expected to proceed with reimbursement listing next month.Janssen Korea is continuing to expand the approved indications for Darzalex SC. Last April, the drug additionally received approval for 3 new indications, including combination therapy with bortezomib, lenalidomide, and dexamethasone (DVRd) for newly diagnosed transplant-eligible multiple myeloma patients. Accordingly, further applications for reimbursement expansion are expected.The reimbursement appropriateness for GSK’s myelofibrosis treatment Omjjara Tab was recognized at this year’s first DREC meeting for “treatment of intermediate- or high-risk myelofibrosis with anemia in adults,” provided that the price is set below the evaluation threshold.Omjjara passed the Cancer Drug Deliberation Committee in March last year, but submission to the reimbursement evaluation committee was delayed due to issues such as the selection of comparator drugs. After approximately 10 months, it was resubmitted and cleared the first hurdle at this year’s DREC meeting.Like Darzalex SC, it entered NHIS drug price negotiations in March and ultimately reached a final agreement. Reimbursement listing is scheduled for next month.Meanwhile, negotiations for Mounjaro, which entered price negotiations in January this year, broke down. Although the company applied for the flexible pricing contract system, it is reported that the parties reportedly failed to narrow differences regarding the separately negotiated amount.

- Policy
- Multi-listing rule hits non-innovative companies harder
- by Jung, Heung-Jun May 19, 2026 11:08am
- The ‘multi-product listing management’ rule, introduced to prevent excessive proliferation of generics, will operate far more harshly against non-innovative companies.While innovative and quasi-innovative companies will receive a three-year grace period, general companies will face immediate price cuts to 30.6%-38.5%, depending on whether they pass bioequivalence testing, leading to a significant widening of the price gap.According to industry sources on the 18th, the impact of the multi-product listing penalty system, newly introduced starting this August, will differ dramatically depending on a company’s innovation classification.Impact of the multi-product listing penalty systemThe Ministry of Health and Welfare recently issued an administrative notice revising the “Standards for Drug Price Determination and Adjustment,” newly introducing a provision applying 85% of the calculated price once the total number of identical formulations reaches 14 or more. Drugs eligible for additional premiums will also be subject to the 85% rule once the premium period ends.For innovative and quasi-innovative companies, the drug price premium period is 1+3 years if domestic manufacturing conditions are met. In other words, a 3-year grace period applies to the multi-product listing penalty as well.In contrast, general companies face an immediate reduction from the standard calculation rate of 45% to 38.25% once the number of listed products exceeds 14. If they failed to conduct their own bioequivalence testing, the price is reduced by an additional 20%, falling to 30.6%.For example, if a generic drug with an original product price of KRW 1,000 reaches 14 or more listed generics, an innovative company would maintain a price of KRW 600 won, reflecting a 60% premium, for four years before eventually dropping to KRW 382.5. A quasi-innovative company would maintain KRW 500 under a 50% premium for four years before dropping to KRW 382.5.However, the generic drug of a general company would sell at KRW 450 for only one year under the standard calculation rate before falling to KRW 382.5.This means that while innovative and quasi-innovative companies maintain prices of KRW 500–600 for three years by meeting domestic manufacturing requirements, general companies immediately face deteriorating profitability at KRW 382.5.If an ordinary company additionally failed to meet the bioequivalence testing requirement, the price would fall to KRw 306, creating nearly a twofold price gap compared with innovative companies.Ultimately, this structure ensures that the penalty for listing multiple products is applied more strictly to general companies, and a sales gap with innovative and quasi-innovative companies is inevitable during the grace period for the price adjustment.In effect, general companies effectively lose the advantage of product listing after the 14th generic entrant, subject to the multi-product pricing rule, enters the list.
- Policy
- Price cuts on existing drugs divided into two phases
- by Jung, Heung-Jun May 18, 2026 09:11am
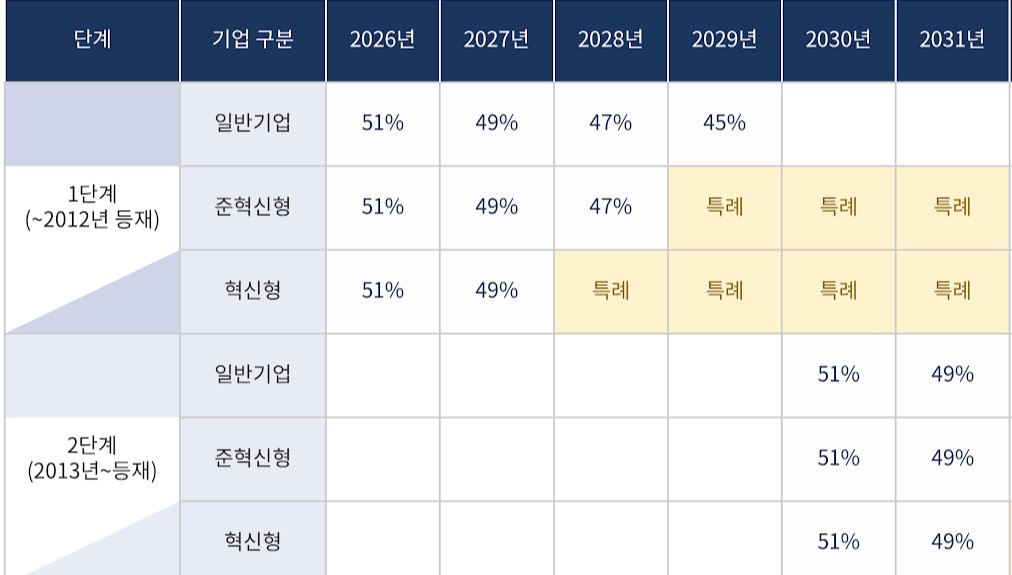
- As the government proceeds with planned pharmaceutical pricing system reforms, follow-up discussions are expected regarding specific classification criteria for price reductions of pre-listed drugs.Key issues include how to distinguish between first-phase and second-phase price reductions for two- and three-drug combination products, as well as how and when later bioequivalence testing should be reflected in drug price reductions.According to industry sources on the 15th, specific criteria for price reductions on pre-listed drugs have not yet been finalized. Discussions on price reductions for pre-listed drugs were not properly addressed during the working-level consultative body meeting between the government and the pharmaceutical industry held in late April.Previously, the Health Insurance Review and Assessment Service (HIRA) decided to divide drugs into two groups based on their listing date in 2012. Price reductions for ingredients listed before 2012 will begin immediately within this year, while reductions for Phase 2 drugs, listed after 2012, will begin in 2030.The timing of implementation differs depending on whether a product is classified into the first or second phase of existing drug price cutsHowever, opinions remain divided regarding the classification of combination products. If the individual ingredients making up a combination drug belong to both Phase 1 and Phase 2 groups, authorities must determine at which timing the combination product itself will face price reductions.The government has stated that if even one ingredient in a combination product was listed before 2012, the combination drug would be classified as a Phase 1 drug.However, there are many issues that require consultation with the industry, such as how to handle cases where even a single ingredient retains a patent or has PMS remaining.Another key issue is how to reduce prices for drugs that failed to meet required standards due to a lack of bioequivalence testing. The reduction rate under the differentiated standards system has been increased from 15% to 20%.For example, if a product price was lowered to 45% and bioequivalence testing was not conducted, it would fall further to 36%. If a rate of 49% is applied, being a product from an innovative pharmaceutical company, it would become 39.2%, while applying a quasi-innovative rate of 47% would drop the price to 37.6%.Since price reductions for pre-listed drugs are implemented over a 10-year period, including a grace period, it is also important to determine how to reflect the results if bioequivalence testing is conducted during that period.In particular, since Phase 2 drugs will only begin facing reductions in 2030, some pharmaceutical companies may attempt to protect reduction rates by conducting bioequivalence studies.Accordingly, industry players are expected to argue that satisfying bioequivalence requirements by the final year converging toward the calculation rate should still qualify as meeting standard requirements.

- Policy
- Calculation rate for generic drug prices set at 45%
- by Lee, Jeong-Hwan May 18, 2026 09:11am
- The government has announced that a drug pricing reform plan, which cuts the drug price calculation rate for currently listed generics from 53.55% to 45%, will take effect on August 1st.The reform plan also includes improvements regarding the management of multiple-listed items, drug price calculations for transfers and acquisitions, support criteria for drugs subjected to market withdrawal, and criteria for semi-innovative pharmaceutical companies.On the 14th, the Ministry of Health and Welfare (MOHW, Minister Jung Eun-kyeong) issued a public notice for the partial amendment to the "Criteria for determination and adjustment of drugs." The ministry plans to finalize the amendment after gathering public feedback by July 13th.The implementation date for the drug pricing reform specified in the amendment notice is August 1st. The government announced that it will gather opinions until July 13th.Generic drug price calculation rate 45%....products failing to meet requirements will be priced below 36%First, the drug price calculation rate for currently listed generics will be reduced from 53.55% to 45%. The calculation rate applied to generics that fail to meet the baseline requirements will also be reduced from 85% to 80%.The baseline requirements for the drug price include whether the company conducted an independent bioequivalence test and whether it used registered drug master file (DMF) ingredients.Generics that meet all baseline requirements will be priced at 45%, those meeting some requirements will be priced at 36%, and products failing to meet any requirements will be priced at 29%.In the case of tiered pricing, the price will be cut once the number of listed items with the same formulation exceeds 13. This is a tighter restriction compared to the current threshold of 20 or more items.If the sum of the newly applied product and the number of currently listed items with the same formulation exceeds 14, the upper limit price will be fixed at 85% of the calculated amount once the price premium period ends.Innovative pharmaceutical companies, semi-innovative pharmaceutical companies, and supply-stabilizing leading pharmaceutical firms will receive preferential drug pricing. Among drugs that meet all baseline requirements, items from innovative pharmaceutical companies will receive a 60% price premium. The premium rate for items from semi-innovative pharmaceutical companies or supply-stabilizing leading pharmaceutical companies will be 50%.Definitions for semi-innovative pharmaceutical companies and supply-stabilizing leading pharmaceutical companies were also established. A supply-stabilizing leading pharmaceutical company is defined as a firm whose ratio of low-profit prevention support drugs, or the ratio of billing amounts among its listed drugs, is 20% or higher.Regarding transfers and acquisitions, the government decided to restrict the succession of existing upper limit prices for items involving a change in a manufacturer's status, excluding inheritance or mergers. Even if a generic item that maintains a high drug price is acquired, the recalculated drug price will be applied from the time of the transfer and acquisition.This regulation is designed to block back-door strategies to evade drug price cuts by purchasing items that maintain high prices.Support for drugs facing production discontinuation will be strengthened. The designation criteria for these drugs are KRW 578 for oral medications, KRW 44 per minimum unit for oral liquids, KRW 3,080 for external preparations, and KRW 5,783 for injections.A new premium clause was also created for pharmaceutical companies that have contributed to supply stabilization. The premium evaluation items include the track record of stable supply fulfillment, national essential medicines, single-listed medicines, low-priced medicines, the use of domestically produced raw ingredients, an annual billing amount of less than KRW 500 million in the previous year, treatments for statutory infectious diseases, and infectious disease crises or urgent supply shortage situations.Price-volume linkage system officiated…implemented on April 1st and October 1st of each yearThe timing of drug price cuts resulting from the price-volume linkage system and the expansion of the scope of use has been unified. The amendment specified that the ex officio adjustment of the upper limit price of drugs will be implemented on April 1st and October 1st of each year, unless there are special circumstances.In addition, a basis was established for pharmaceutical companies to refund the increased expenditure on health insurance incurred during the implementation grace period to the National Health Insurance Service if a drug price adjustment is issued at a time other than the regular implementation date.Meanwhile, the MOHW plans to implement the announced reform plan on August 1st. Regulations related to the regularization of the price-volume linkage will apply starting in January of next year (2027). The first regular drug price adjustment will take effect on April 1st, 2027.
- Policy
- Merck’s two new rare disease drugs receive GIFT designation
- by Lee, Tak-Sun May 15, 2026 02:44pm
- AI-generated imageThe Ministry of Food and Drug Safety (MFDS) is speeding up domestic approval timelines by designating two rare disease treatments from Merck as subjects for Korea’s Global Innovative products on Fast Track (GIFT) program.The MFDS announced that it designated Merck’s desmoid tumor treatment ‘Ogsiveo Tab’ and tenosynovial giant cell tumor (TGCT) treatment ‘Pimicotinib Cap’ as the 70th and 71st GIFT products, respectively. This designation is a measure to support the expedited approval of new drugs from innovative pharmaceutical companies that either have no existing treatment options or have demonstrated improved efficacy and safety.Ogsiveo Tab (nirogacestat hydrobromide), which was designated as a GIFT product on April 21, is a treatment for adult patients with desmoid tumors requiring systemic therapy. The drug suppresses tumor growth by inhibiting gamma secretase (GS) and blocking Notch signaling pathways.The drug has already received approval from the US FDA (November 2023) and the European EMA (August 2025), and was designated as an orphan drug in Korea on February 24, 2026. The MFDS selected it for expedited review based on the lack of existing treatment options.Then, on April 27, “Pimicotinib Cap (pimicotinib hydrochloride monohydrate),” a treatment for tenosynovial giant cell tumor(TGCT), was added to the GIFT list. The treatment works by selectively inhibiting the colony-stimulating factor-1 receptor (CSF-1R) to block disease progression.Pimicotinib is currently under development with FDA Fast Track and Breakthrough Therapy Designation (BTD) status in the United States, but has not yet received full approval in any global market. MFDS acknowledged the drug’s potential efficacy improvements and decided to manage it as a fast-track review product.The two products designated under GIFT will benefit from review periods shortened by approximately 25% compared to standard reviews. In addition, a rolling review of prepared materials and customized consultations with professional reviewers prior to the submission of the marketing authorization application will be provided, which is expected to significantly accelerate the timeline for the drug’s introduction in Korea.An MFDS official stated, “The exact indications and efficacy will be finalized after reviewing the submitted data. We will spare no effort in the review process to ensure that patients with intractable rare diseases can be provided with new treatment opportunities as quickly as possible.”