- LOGIN
- MemberShip
- 2026-06-15 15:44:34
- A numbers-driven look into Korea's reimbursement system
- by Son, Hyung Min | translator Alice Kang | 2026-06-15 09:18:59

It is no exaggeration to say that today's pharmaceutical market is defined by ‘reimbursement,’ no matter how strong the momentum behind new obesity drugs may be.
Reimbursement listing and how quickly it is obtained ultimately determines the commercial success of a new medicine. Amid a flood of high-cost drugs with multiple indications, pharmaceutical market access (MA) professionals have become some of the industry's most sought-after specialists.
Oncology drugs sit at the center of this trend. Cancer drug development is increasingly moving beyond single-cancer indications, with therapies expanding into multiple tumor types and treatment settings. Immuno-oncology drugs initially developed for lung cancer, for example, are now being used in gastric cancer, esophageal cancer, triple-negative breast cancer (TNBC), endometrial cancer, and renal cell carcinoma.
Cancer treatment, which has been focused on end-stage disease management, has evolved to be used in neoadjuvant and adjuvant settings, for recurrence prevention, and as maintenance therapy, fundamentally reshaping treatment strategies.
The challenge, however, is their reimbursement. A new oncology drug must pass through multiple stages before obtaining reimbursement coverage, including review by the Cancer Disease Deliberation Committee (CDDC), the Drug Reimbursement Evaluation Committee (DREC), price negotiations with the National Health Insurance Service (NHIS), and final approval by the Health Insurance Policy Deliberation Committee (HIPDC).
Among these, the Cancer Disease Deliberation Committee serves as the first gateway to reimbursement. As it is the first and most critical gateway that determines reimbursement potential, the committee is often referred to as a "wall of lamentation" by companies with oncology products.
Only half of approved oncology drugs passed final review during the past 3.5 years
Even among drugs that received positive CDDC reviews, only 65.2% ultimately reached reimbursement listing after completing NHIS price negotiations and HIPDC review.
An analysis conducted by DailyPharm on the Cancer Disease Deliberation Committee and Drug Reimbursement Evaluation Committee decisions between January 2023 and June 2026 found that only 65.2% of indications that passed reimbursement evaluation ultimately succeeded in obtaining reimbursement listing.
During the same period, the Cancer Disease Deliberation Committee reviewed a total of 244 oncology drug indications. Of these, 124 indications (50.6%) received reimbursement criteria. On the other hand, 86 indications (35.2%) were denied reimbursement criteria, and 34 indications (13.9%) were sent back for reconsideration.
In other words, only 1 out of every 2 oncology indications successfully cleared the first committee.
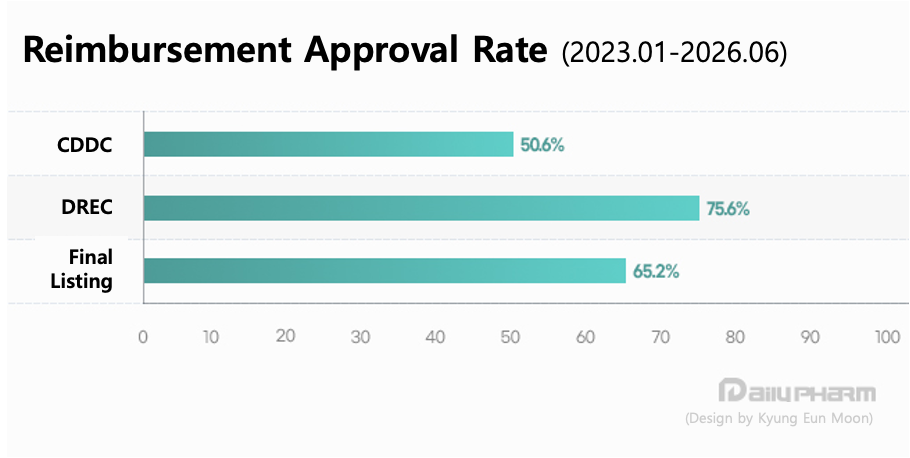
By contrast, approval rates at the DREC level were considerably higher. Over the past 3 years, the committee reviewed 81 oncology indications, of which 59 received reimbursement adequacy approvals, resulting in an approval rate of 75.6%. Meanwhile, 9 indications (11.1%) were reconsidered, and 13 indications (16.0%) were deemed not appropriate for reimbursement. Ultimately, 65.2% eventually completed NHIS negotiations and secured reimbursement listing (excluding results from the 6th meeting of 2026).
The time required to complete the reimbursement process also remains a significant issue. According to the Korea Alliance of Patient Organizations, the average period from regulatory approval to reimbursement listing for 32 oncology drugs listed between 2021 and 2025 was 659 days. This means patients waited an average of 1 year and 10 months after approval before gaining access to reimbursement benefits.
Experts attribute these delays to redundant reviews of clinical value and budget impact that occur throughout the reimbursement process, from CDDC and DREC review, price negotiations, to HIPDC review.
MSD makes the most attempt at reimbursement… Multi-indication development accelerates
Among pharmaceutical companies, MSD was the most active in pursuing reimbursement expansion. Over the past three years, 44 MSD-related oncology indications were reviewed, the highest number among all companies. Most of these reviews involved expanding reimbursement for its immuno-oncology drug Keytruda (pembrolizumab).
MSD was followed by Janssen (28), Roche (17), Pfizer and Lilly (10 each), Astellas (9), and AstraZeneca (8).
Blockbuster oncology products such as ‘Darzalex (daratumumab),’ ‘Rybrevant (amivantamab),’ ‘Enhertu (trastuzumab deruxtecan),’ and ‘Tevimbra (tislelizumab)’ have repeatedly appeared before both the CDDC and DREC as their indications expanded across multiple cancer types and treatment settings.
This trend reflects more than simply an increase in the number of reimbursement applications submitted by individual companies. It demonstrates a broader shift in the oncology drug development paradigm toward a multi-indication model.
Rather than remaining confined to a single cancer type, new oncology drugs are increasingly expanding into early-stage and metastatic settings, combination regimens, and biomarker-defined patient populations. As a result, repetitive and ongoing reimbursement reviews have been ongoing for a single new drug.
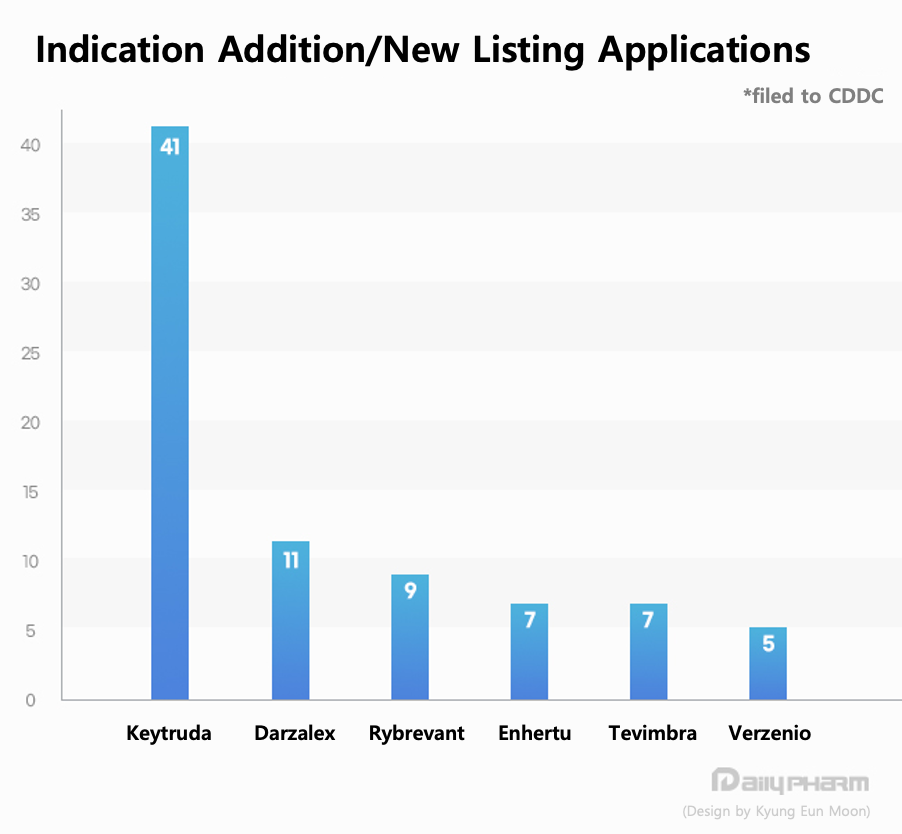
Among individual products, Keytruda was the most active. Over the past 3 years, Keytruda has pursued reimbursement expansion across 11 solid tumor indications, including lung cancer, gastric cancer, esophageal cancer, triple-negative breast cancer (TNBC), cervical cancer, endometrial cancer, and renal cell carcinoma. More specifically, the drug underwent review for a total of 41 indications.
This reflects the rapid expansion of immuno-oncology therapies from an initial focus on metastatic cancers into neoadjuvant and adjuvant settings, biomarker-based populations, and combination therapies.
Following Keytruda, the products with the highest number of reviews were Darzalex (11 indications), Rybrevant (9), Enhertu and Tevimbra (7 each), Verzenio (abemaciclib, 5), Columvi (glofitamab), 4), Polivy (polatuzumab vedotin, 4), Padcev (enfortumab vedotin, 4), and Opdivo (nivolumab) (4)
Efforts to expand reimbursement coverage also continued in rare cancers. ‘Welireg (belzutifan)’ sought reimbursement for indications including Von Hippel-Lindau (VHL) disease-associated renal cell carcinoma and metastatic renal cell carcinoma (mRCC). However, discussions were prolonged because of the limited patient population and cost-effectiveness concerns.
In particular, immuno-oncology therapies are considered the fastest-growing category in terms of indication expansion. Products such as Keytruda, Opdivo, and Tevimbra are extending beyond metastatic disease into earlier treatment settings and combination regimens, leading to broader reimbursement discussions. On the other hand, expanding patient populations and the potential for longer treatment durations have made reimbursement decisions increasingly complex for both the CDDC and DREC.
Rybrevant, Verzenio, and Welireg…still await review at CDDC stage
A considerable number of products repeatedly faced either the non-establishment of reimbursement criteria or requests for reconsideration.
The product with the highest number of such cases was Keytruda. Over the past 3 years, Keytruda accumulated 30 indications that were either denied reimbursement criteria or sent back for reconsideration. Given the rapid pace of indication expansion, reimbursement discussions were repeatedly revisited.
Rybrevant and Darzalex each experienced 8 indications that were either reconsidered or denied reimbursement criteria. Rybrevant repeatedly sought reimbursement expansion in areas of high unmet need, including EGFR exon 20 insertion-mutated non-small cell lung cancer and first-line combination therapy settings. However, many of these indications failed to advance to the reimbursement-criteria establishment stage.
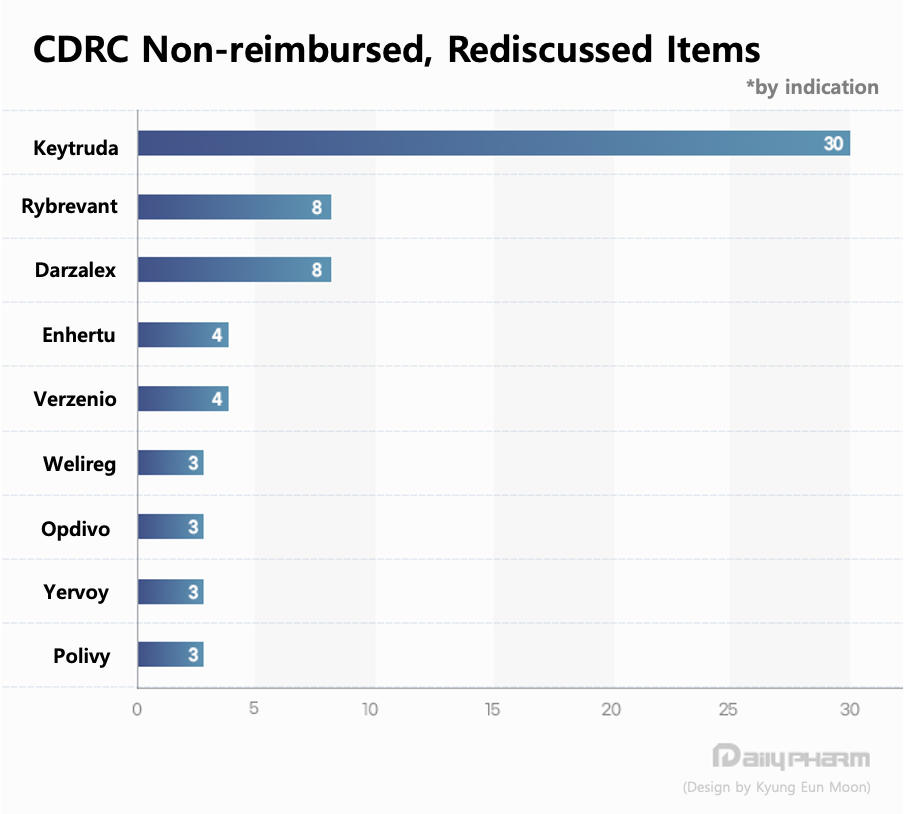
Enhertu and Verzenio each recorded 4 indications, and Welireg, Opdivo, Yervoy (ipilimumab), and Polivy each had 3 indications that failed to secure reimbursement criteria or were sent back for further review.
For Verzenio, repeated reimbursement discussions centered on adjuvant treatment for HR-positive/HER2-negative early breast cancer, where the balance between recurrence prevention benefits and cost-effectiveness became a major issue. For Welireg, discussions were prolonged because of the combination of a small patient population, limited clinical evidence, and cost-effectiveness concerns.
Ultimately, the results of the past 3 years suggest that Korea's oncology reimbursement system has struggled to keep pace with the rapid expansion of approved indications.
With more therapies quickly expanding into multiple indications, like immunotherapies and antibody-drug conjugates (ADCs), reimbursement decisions are becoming increasingly complex. Finding the appropriate balance between patient access and the long-term sustainability of the National Health Insurance system is expected to remain a central challenge for future discussions within both the CDDC and DREC.
A 50% pass rate: the gap between regulatory approval and reimbursement
Looking solely at recent figures, the CDDC has emerged as the highest hurdle within Korea's oncology reimbursement framework.
The committee does not merely assess whether a drug has received regulatory approval. Rather, it determines the actual scope of reimbursement criteria and conditions of use, taking into account clinical need, availability of alternative treatments, target patient populations, and budget impact. By contrast, DREC primarily reviews indications that have already passed CDDC review and focuses on cost-effectiveness, budget impact, and the potential applicability of risk-sharing agreements (RSAs).
As a result, many observers argue that reimbursement outcomes for oncology drugs are largely determined at the CDDC stage. On-site, there has been criticism that considerations such as budget impact and cost-effectiveness exert substantial influence during the reimbursement-criteria setting process, limiting early patient access even to therapies that have become the global standard of care.
The increasing use of adjuvant therapy in early-stage cancer has further complicated reimbursement discussions. As immunotherapies, targeted therapies, and CDK4/6 inhibitors are increasingly used after surgery to reduce recurrence risk, the question, “To what extent should recurrence prevention be recognized as a reimbursable clinical benefit?” has arisen as the new point of concern.
Opinions remain divided regarding the CDDC’s relatively low approval rate. Some healthcare professionals argue that as oncology drugs expand into new indications at an accelerating pace, financial and cost-effectiveness considerations are being introduced too early in the reimbursement process. However, committee experts contend that prioritization is unavoidable given the constraints of a limited national health insurance budget.
One committee member explained that reimbursement decisions for oncology drugs cannot be based solely on efficacy. Rather, they require a complex assessment that incorporates treatment outcomes, quality of life, and long-term financial sustainability.
The member explained, "Patients would naturally want access to effective treatments as quickly as possible. However, because the national health insurance system is funded by public resources, cost-effectiveness is a must. As high-cost oncology drugs become more expensive and expand into more indications, we inevitably apply stricter standards when assessing which patient populations derive meaningful value from treatment."
Even when differences in survival are modest, treatments that reduce toxicity and preserve quality of life can still provide meaningful benefits. Nevertheless, priorities must ultimately be established within budget constraints. The reimbursement process for oncology drugs is fundamentally about finding a balance between clinical value and financial sustainability."
Many clinicians, however, see the situation differently. They argue that reimbursement discussions are failing to keep pace with the speed of clinical innovation.
One medical oncologist noted, “Patients who experience recurrence often require longer treatment durations and sequential use of multiple therapies, which ultimately increases socioeconomic costs. Reducing the risk of recurrence early and maintaining patients in a healthy state for longer periods has value not only for individual patients but also from a long-term healthcare financing perspective."
“Rather than granting reimbursement to all therapies, the more important task is identifying which patient populations derive the greatest clinical value. Ultimately, oncology reimbursement policy is about balancing short-term costs against long-term treatment value. Adjusting the current 5% patient co-insurance rate could also be one possible approach."
-

- 0
댓글 운영방식은
댓글은 실명게재와 익명게재 방식이 있으며, 실명은 이름과 아이디가 노출됩니다. 익명은 필명으로 등록 가능하며, 대댓글은 익명으로 등록 가능합니다.
댓글 노출방식은
댓글 명예자문위원(팜-코니언-필기모양 아이콘)으로 위촉된 데일리팜 회원의 댓글은 ‘게시판형 보기’와 ’펼쳐보기형’ 리스트에서 항상 최상단에 노출됩니다. 새로운 댓글을 올리는 일반회원은 ‘게시판형’과 ‘펼쳐보기형’ 모두 팜코니언 회원이 쓴 댓글의 하단에 실시간 노출됩니다.
댓글의 삭제 기준은
다음의 경우 사전 통보없이 삭제하고 아이디 이용정지 또는 영구 가입제한이 될 수도 있습니다.
-
저작권·인격권 등 타인의 권리를 침해하는 경우
상용 프로그램의 등록과 게재, 배포를 안내하는 게시물
타인 또는 제3자의 저작권 및 기타 권리를 침해한 내용을 담은 게시물
-
근거 없는 비방·명예를 훼손하는 게시물
특정 이용자 및 개인에 대한 인신 공격적인 내용의 글 및 직접적인 욕설이 사용된 경우
특정 지역 및 종교간의 감정대립을 조장하는 내용
사실 확인이 안된 소문을 유포 시키는 경우
욕설과 비어, 속어를 담은 내용
정당법 및 공직선거법, 관계 법령에 저촉되는 경우(선관위 요청 시 즉시 삭제)
특정 지역이나 단체를 비하하는 경우
특정인의 명예를 훼손하여 해당인이 삭제를 요청하는 경우
특정인의 개인정보(주민등록번호, 전화, 상세주소 등)를 무단으로 게시하는 경우
타인의 ID 혹은 닉네임을 도용하는 경우
-
게시판 특성상 제한되는 내용
서비스 주제와 맞지 않는 내용의 글을 게재한 경우
동일 내용의 연속 게재 및 여러 기사에 중복 게재한 경우
부분적으로 변경하여 반복 게재하는 경우도 포함
제목과 관련 없는 내용의 게시물, 제목과 본문이 무관한 경우
돈벌기 및 직·간접 상업적 목적의 내용이 포함된 게시물
게시물 읽기 유도 등을 위해 내용과 무관한 제목을 사용한 경우
-
수사기관 등의 공식적인 요청이 있는 경우
-
기타사항
각 서비스의 필요성에 따라 미리 공지한 경우
기타 법률에 저촉되는 정보 게재를 목적으로 할 경우
기타 원만한 운영을 위해 운영자가 필요하다고 판단되는 내용
-
사실 관계 확인 후 삭제
저작권자로부터 허락받지 않은 내용을 무단 게재, 복제, 배포하는 경우
타인의 초상권을 침해하거나 개인정보를 유출하는 경우
당사에 제공한 이용자의 정보가 허위인 경우 (타인의 ID, 비밀번호 도용 등)
※이상의 내용중 일부 사항에 적용될 경우 이용약관 및 관련 법률에 의해 제재를 받으실 수도 있으며, 민·형사상 처벌을 받을 수도 있습니다.
※위에 명시되지 않은 내용이더라도 불법적인 내용으로 판단되거나 데일리팜 서비스에 바람직하지 않다고 판단되는 경우는 선 조치 이후 본 관리 기준을 수정 공시하겠습니다.
※기타 문의 사항은 데일리팜 운영자에게 연락주십시오. 메일 주소는 dailypharm@dailypharm.com입니다.